Quiz-summary
0 of 41 questions completed
Questions:
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- 33
- 34
- 35
- 36
- 37
- 38
- 39
- 40
- 41
Information
This quiz will review normal anatomy of the aortic valve as well as pathologies, focusing on stenosis and regurgitation.
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 41 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Categories
- Not categorized 0%
- Aortic Valve 0%
- Normal TEE 0%
- Normal TTE 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- 13
- 14
- 15
- 16
- 17
- 18
- 19
- 20
- 21
- 22
- 23
- 24
- 25
- 26
- 27
- 28
- 29
- 30
- 31
- 32
- 33
- 34
- 35
- 36
- 37
- 38
- 39
- 40
- 41
- Answered
- Review
-
Question 1 of 41
1. Question
What aortic valve cusps are seen here?
Correct
Exactly! You basically always see the right coronary cusp in the long axis (this is true for TTE and TEE.) The other cusp is usually non-coronary but can be left coronary. Looking at the x-plane image here may help cement that concept.
Incorrect
Whoops, not quite! The long axis view always shows the right coronary cusp of the AV, along with either the non-coronary (more often) or the left coronary (sometimes.) Perhaps this x-plane image will help make that more clear. Notice how the x-plane cuts through the right coronary cusp on the bottom. It would basically be impossible to cut through the aortic valve in this view and not capture a portion of the RCC anteriorly. On the other hand, you could rotate so you saw either the NCC or the LCC. Make sense?
-
Question 2 of 41
2. Question
Describe the aortic valve
Correct
Boom, nailed it. Classic bicuspid aortic valve with fusion of the left and right cusps. Fishmouth opening. Don’t forget to check for an aortic coarctation. Nuff said.
Incorrect
Come on, now, you didn’t mean that did you? You know that this is clearly a bicuspid valve with fusion of the RCC and LCC, right? Now go check this patient for an aortic coarctation.
-
Question 3 of 41
3. Question
What view is this and why do we make it?
Correct
Yep, piece of cake.
Incorrect
Nope, not quite. This is the deep transgastric long axis. It looks a little bit like the apical 5 chamber (because it is a little like that, but there’s multiplane in the image.) It’s created by advancing the probe from the transgastric window deeper into the stomach and anteflexing. Hopefully your probe will be somewhere near the apex of the LV and will create an image like this. This is one of 2 views in TEE that can be used to interrogate the AV with spectral doppler. Why can’t we just do spectral doppler from the midesophageal windows?
-
Question 4 of 41
4. Question
Describe the view and the nature of the aortic valve
Correct
Nice job! This is an incredibly rare image of a quadricuspid valve. When you see one, you’re almost certainly wrong. Much more commonly you’re seeing a trileaflet valve with a weird cut, but this was confirmed with direct visualization of the valve.
Incorrect
Nope, this is a parasternal short axis of the AV. And the valve is QUADRICUSIPD, super rare. When you see this you’re almost certainly wrong.
-
Question 5 of 41
5. Question
Name the aortic valve cusps starting at 12 o’clock and moving clockwise
Correct
Nicely done, nothing else to say.
Incorrect
Nope. In this parasternal AV SAX the right ventricle will be at the top of the screen. That makes 12 o’clock the RCC, then the LCC, and the NCC will be at 7 o’clock by the interatrial septum. If this isn’t intuitive because you’re used to the midesophageal RV inflow outflow that’s OK, take a sec to reorient yourself.
-
Question 6 of 41
6. Question
Simple question: is this calcified enough to worry about (should we quantify stenosis) or is it more or less OK?
Correct
Yep, bring the Doppler. This is NOT OK.
Incorrect
Nope, this is not OK. You need to bring the Doppler, this is not mildly stenotic.
-
Question 7 of 41
7. Question
Calculate the aortic valve area
 Correct
Correct
Yep, you got it. Its not rocket science, but it does help to practice.
Incorrect
Nope. I recommend you give that another try until you get it right.
-
Question 8 of 41
8. Question
Bad or not bad?
Correct
Roger that, not too bad. You’d be surprised if this valve had even moderate AS, and certainly there is not severe stenosis.
Incorrect
Nope, not quite. This valve is not so bad. It would be surprising if there was more than mild stenosis, and there is certainly not severe AS.
-
Question 9 of 41
9. Question
Calculate the AVA with an LVOT diameter of 2.2 cm
 Correct
Correct
Yep, piece of cake. Keep up the good work!
Incorrect
Give that another try. Don’t feel badly, it takes practice. Take your time, show your work, and get back in the saddle.
-
Question 10 of 41
10. Question
Worried or not worried?
Correct
You got it, this valve doesn’t open 100% normally but its certainly not bad enough to be significantly stenotic. Well done!
Incorrect
Nope, this isn’t too bad. File this away as “little restricted opening, but not significantly stenotic.”
-
Question 11 of 41
11. Question
Acknowledging the limitations of a single view, how bad is this stenosis?
Correct
You got it, this is moderate aortic stenosis. This should trigger your “Hmm, I’m concerned about this calcification” reaction, but notice that there is some reasonable opening of this valve. It would be totally reasonable to quantify the stenosis here, but you’d be a little surprised if you found severe stenosis.
Incorrect
OK, I know this isn’t a fair question. I just want you to be exposed to a lot of images to build your experience. This should trigger your “Hmm, I’m concerned about this calcification” reaction, but notice that there is some reasonable opening of this valve. It would be totally reasonable to quantify the stenosis here, but you’d be a little surprised if you found severe stenosis.
-
Question 12 of 41
12. Question
How bad do you think the stenosis is?
Correct
Yeah, this is a moderate stenosis situation. Definite limitation of excursion, but probably not enough to kill someone yet. If you wanted to quantify this stenosis that is probably wise, anything you think is moderate or worse should trigger quantification.
Incorrect
Don’t get down, this is a little tough and probably unfair of me to ask. We see here a limitation of excursion, but probably not enough to kill someone yet. If you wanted to quantify this stenosis that is probably wise, anything you think is moderate or worse should trigger quantification.
-
Question 13 of 41
13. Question
Calculate the aortic valve area…
 Correct
Correct
Boom, you nailed it. I know this is straightforward, but you have to be able to do it in your sleep (or at 3:30 in the morning after working all day!)
Incorrect
Whoops, back to the drawing board! Go slow and show your work if you need to.
-
Question 14 of 41
14. Question
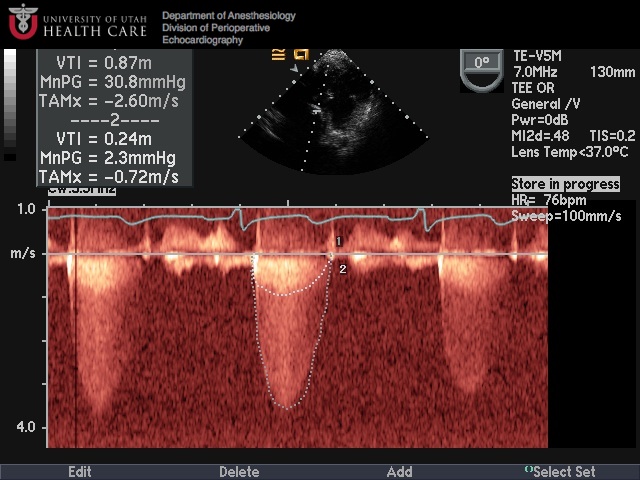
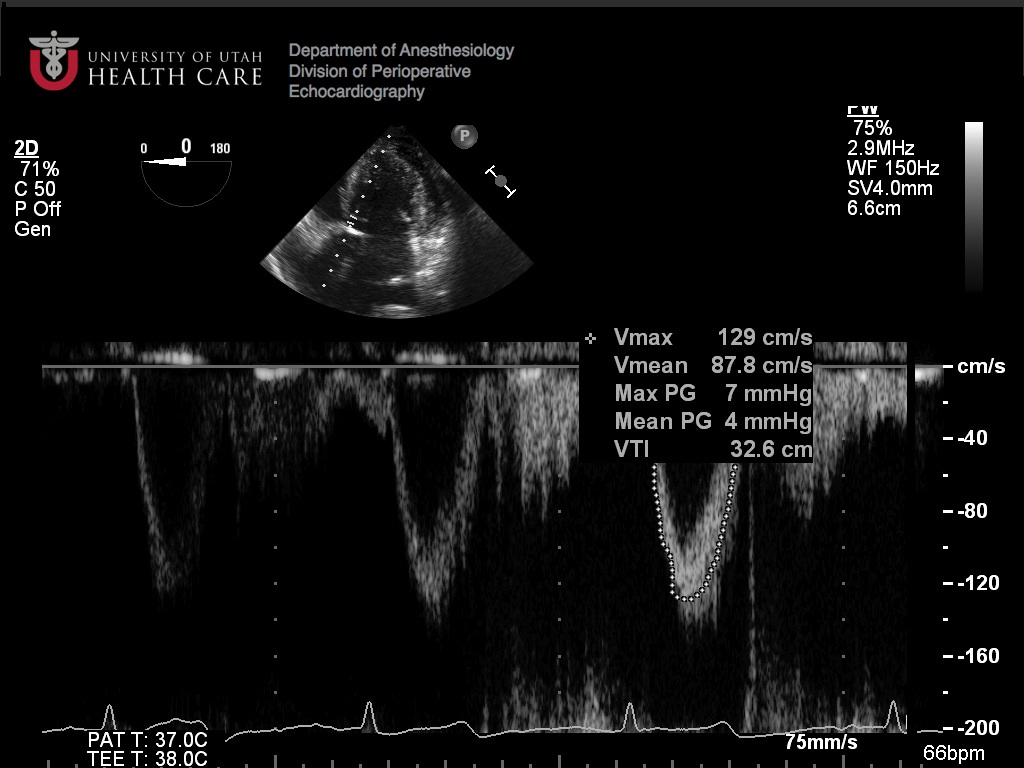
How bad is the aortic stenosis (2 methods)?
 Correct
Correct
Well done, my friend! Continuous wave Doppler through the AV in the deep TG LAX shows us a nice double envelope (remember why that is useful?) We see a peak velocity < 3 (consistent with mild stenosis) and a doppler velocity index of more than 0.5 (also mild.) Both measures are barely on the mild side of moderate, though, so with more quantification you wouldn’t be surprised to find this called “mild-to-moderate.”
Incorrect
Oh darn! Take another look at your quantification of AS if you need to, the American Society of Echo has a nice set of guidelines available on their site (http://www.asecho.org/) In this image, continuous wave Doppler through the AV in the deep TG LAX shows us a nice double envelope (remember why that is useful?) We see a peak velocity < 3 (consistent with mild stenosis) and a doppler velocity index of more than 0.5 (also mild.) Both measures are barely on the mild side of moderate, though, so with more quantification you wouldn’t be surprised to find this called “mild-to-moderate.”
Hint
Nice try, no hints from me. You need to know this stuff, my friend!
-
Question 15 of 41
15. Question
What disease process is causing AV calcification?
Correct
Yep, typical findings of rheumatic aortic valve disease. Good job! In the long axis view there is thickening primarily of the tips of the leaflets. In systole you see the classic “hockey-stick” appearance, especially of the non-coronary cusp here. This is caused by restriction of the tips of the leaflet with relative sparing of the body.
Incorrect
Well, not quite…we’re seeing pretty typical rheumatic disease here. In the long axis view there is thickening primarily of the tips of the leaflets. In systole you see the classic “hockey-stick” appearance, especially of the non-coronary cusp here. This is caused by restriction of the tips of the leaflet with relative sparing of the body.
-
Question 16 of 41
16. Question
What is causing the aortic stenosis?
Correct
Exactly, classic rheumatic aortic valve disease. Well done! In the long axis view there is thickening of the tips of the leaflets. In systole you see the classic “hockey-stick” appearance, especially of the non-coronary cusp here. This is caused by restriction of the tips of the leaflet with relative sparing of the body. You also see dilation of the ascending aorta, which you find associated with aortic stenosis.
Incorrect
We’ll just assume your keyboard is malfunctioning. This is another classic rheumatic valve. In the long axis view there is thickening of the tips of the leaflets. In systole you see the classic “hockey-stick” appearance, especially of the non-coronary cusp here. This is caused by restriction of the tips of the leaflet with relative sparing of the body. You also see dilation of the ascending aorta, which you find associated with aortic stenosis.
Hint
You know me better than that. Get to work!
-
Question 17 of 41
17. Question
What is causing the aortic stenosis?
Correct
Boom, nailed it! This is a classic rheumatic aortic valve. You can see thickening and calcification of the commisures and the tips of the leaflets.
Incorrect
I assume you’re joking…this is a classic rheumatic aortic valve. You can see thickening and calcification of the commisures and the tips of the leaflets. Take a moment to store this in your CPU.
Hint
Not a chance!
-
Question 18 of 41
18. Question
What is causing the aortic stenosis? Are you worried?
Correct
Perfect! This is a degenerative calcification case, with a heavily calcified valve. You expect severe stenosis here.
Incorrect
Nope, back to the drawing board. This is a calcified trileaflet valve, consistent with “degenerative changes” meaning this is not a rheumatic valve. There is calcification throughout the entire body of the leaflet, and there’s a lot of it. You expect severe calcification.
Hint
Not gonna happen! Either you know it or you don’t.
-
Question 19 of 41
19. Question
What is causing the aortic stenosis? Are you concerned or is this no big deal?
Correct
Exactly, nice. This is a heavily calcified (concerning!) aortic valve, with calcification throughout the body of the leaflets consistent with degenerative changes of aging and decrepitude.
Incorrect
Bzzzt! Try again! This is a heavily calcified (concerning!) aortic valve, with calcification throughout the body of the leaflets consistent with degenerative changes of aging and decrepitude.
-
Question 20 of 41
20. Question
What does the first image suggest about aortic valve function? Does the second image refute this?
Correct
Exactly, well done. The color flow signal suggests only mild AI, you would be surprised if it was more. The continuous wave Doppler confirms this with a pressure half time above 500 ms (the cutoff below which we call AI moderate.)
Incorrect
Take another look at this and regroup. The color flow signal in the parasternal LAX suggests only mild AI, you would be surprised if it was more. The continuous wave Doppler confirms this with a pressure half time above 500 ms (the cutoff below which we call AI moderate.)
-
Question 21 of 41
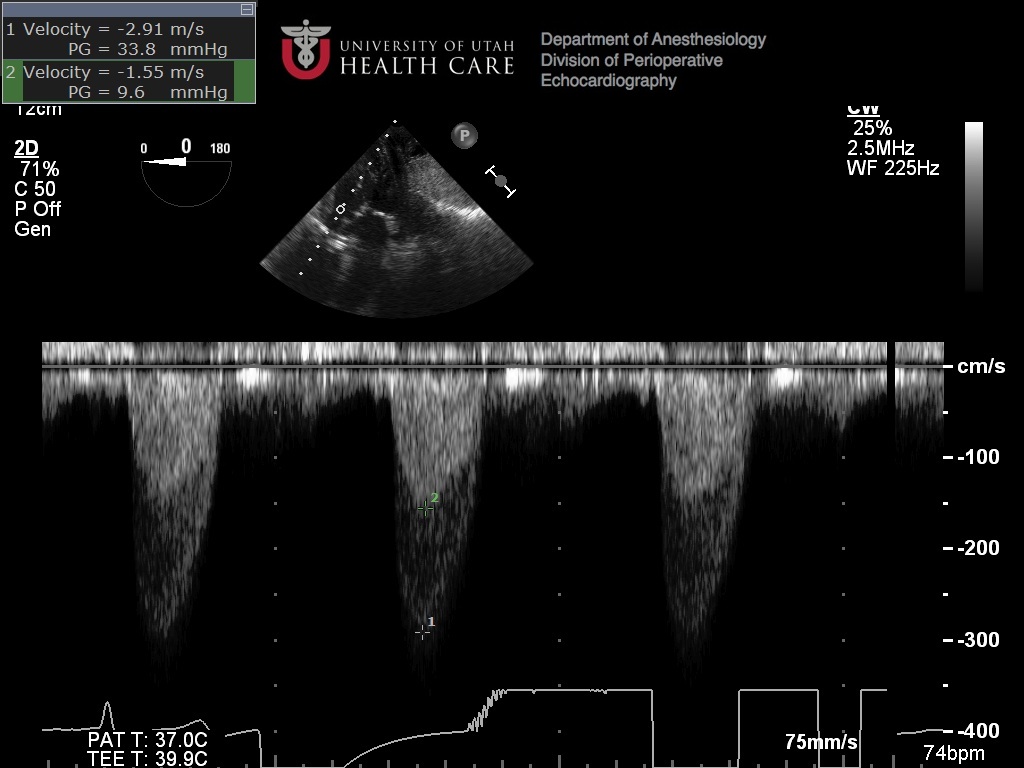
21. Question
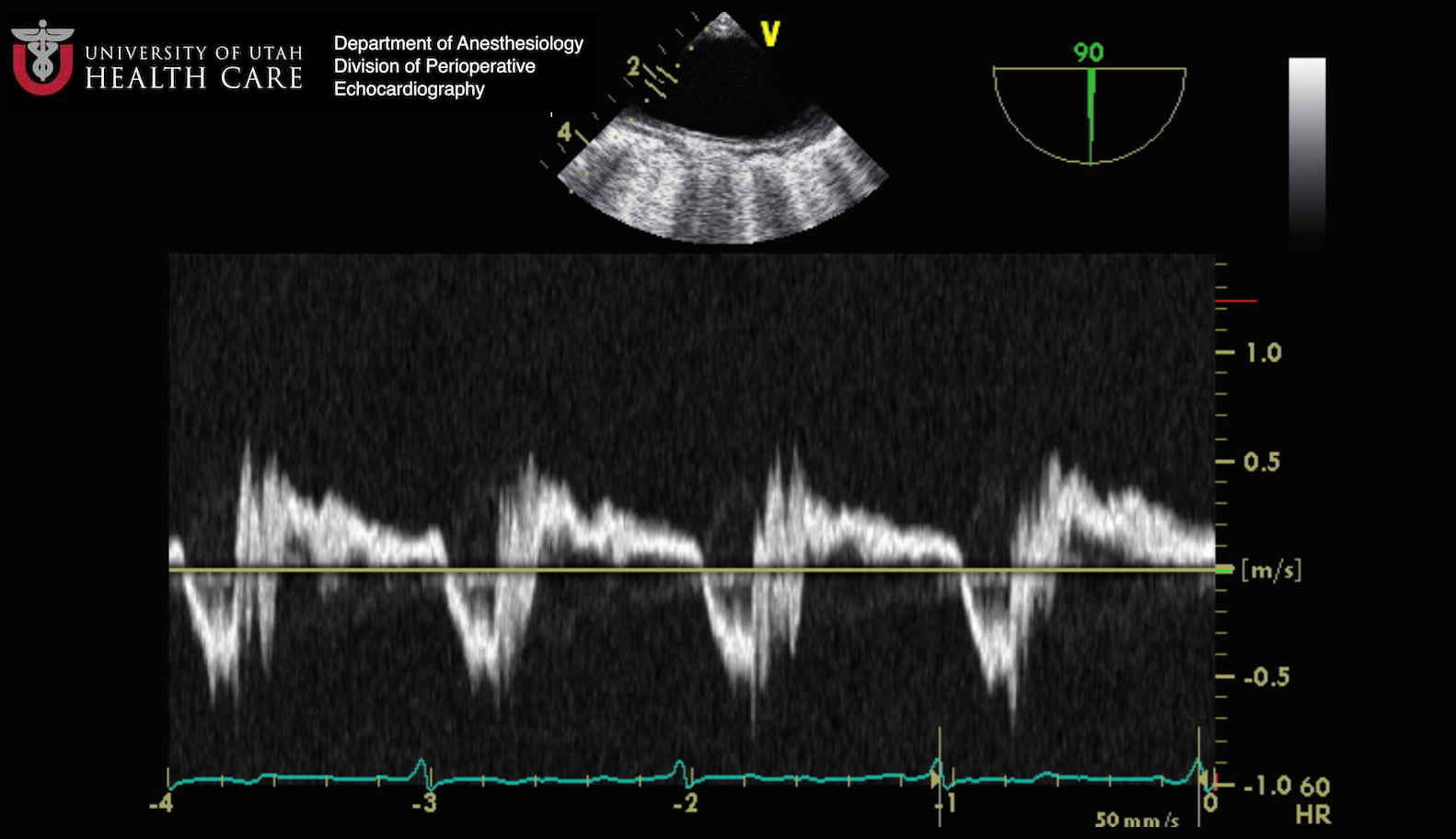
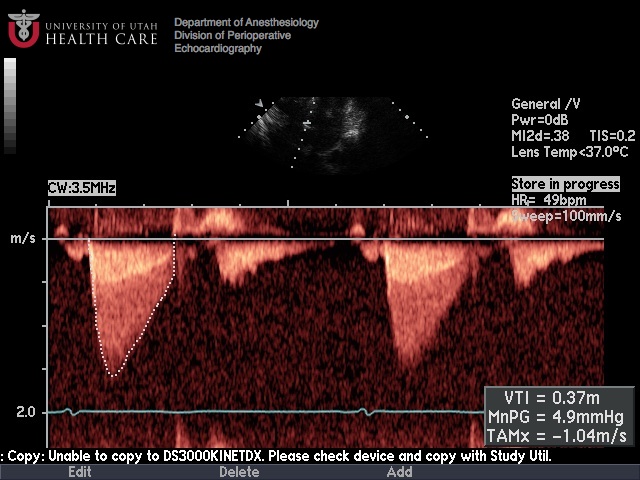
What are we seeing here and what does it mean?
Correct
Yep, exactly! This is holodiastolic reversal of flow in the thoracic aorta (notice the high velocity of the diastolic signal as well.) You expect this to be the descending aorta rather than the arch because of the long axis appearance in the scout image at 90 degrees. This is a specific finding for severe aortic insufficiency.
Incorrect
I’m sure you’re on the right track. This is holodiastolic reversal of flow in the thoracic aorta (notice the high velocity of the diastolic signal as well.) You expect this to be the descending aorta rather than the arch because of the long axis appearance in the scout image at 90 degrees. This is a specific finding for severe aortic insufficiency.
-
Question 22 of 41
22. Question
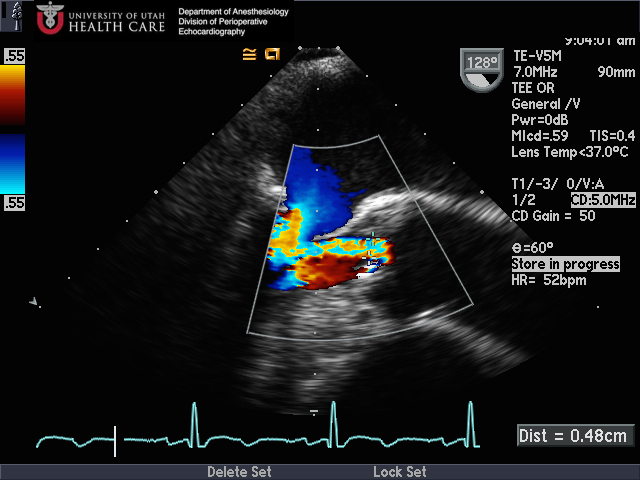
What view is this? Concerning or not?
Correct
Yeah, you got it! This is a parasternal SAX of the aortic valve with color flow. You had better be concerned about all the flow you see in diastole. This patient has severe aortic insufficiency.
Incorrect
Nope, not exactly. Try again and I’m sure you’ll get it. This is a parasternal SAX of the AV with significant color flow seen in diastole. This should concern you for significant aortic insufficiency.
-
Question 23 of 41
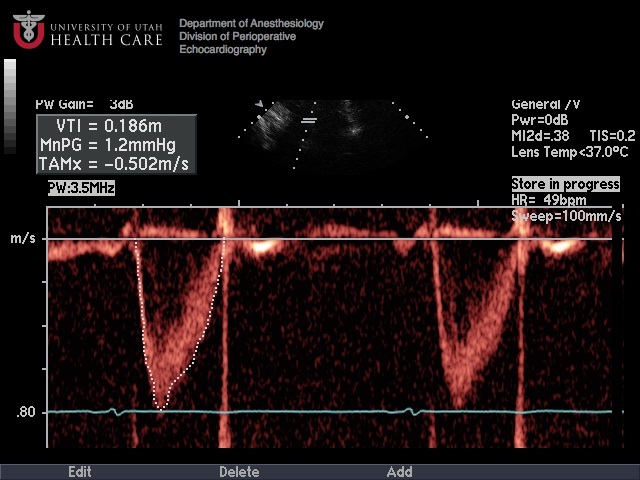
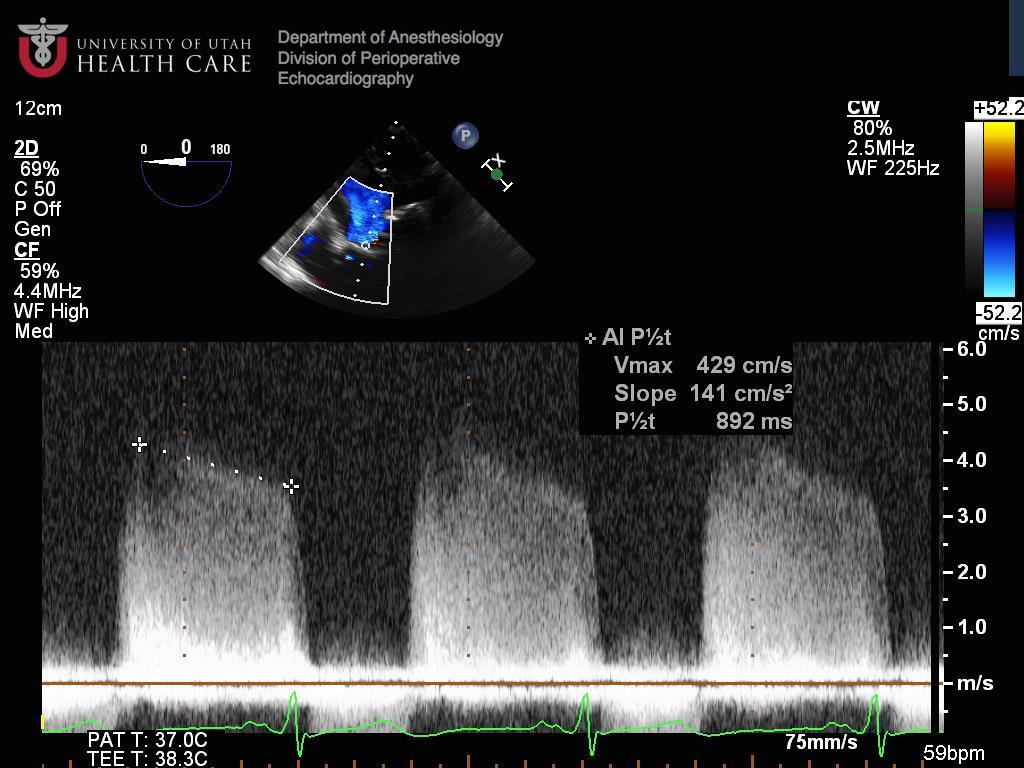
23. Question
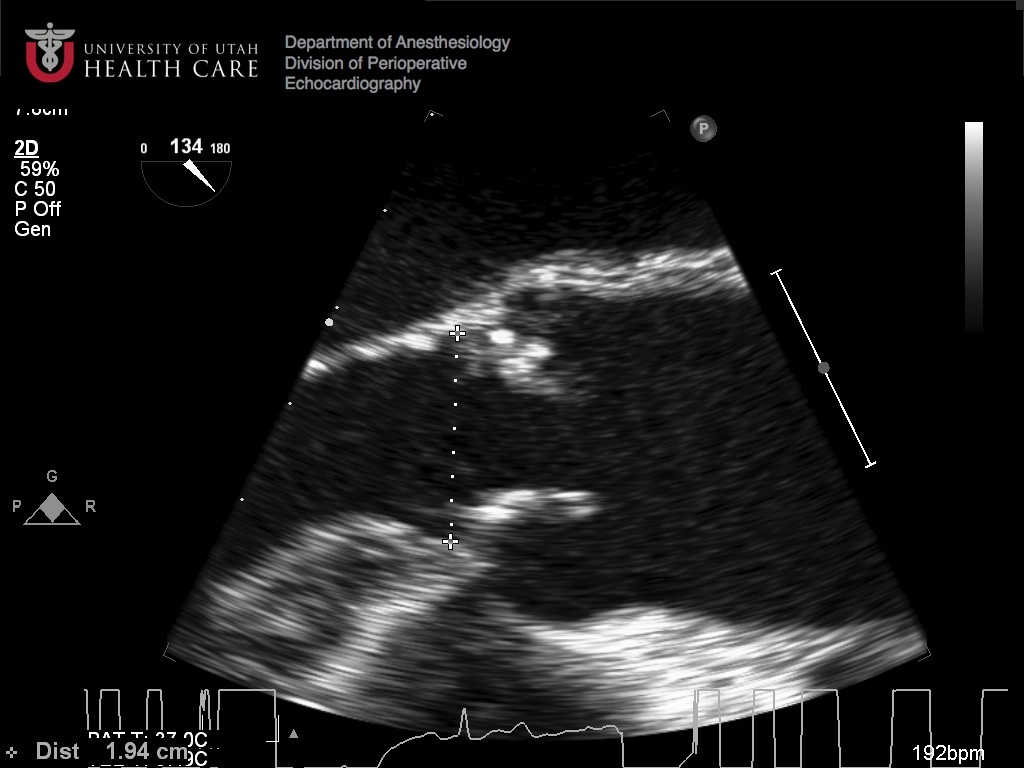
If this were all the information you had, how would you quantify the aortic insufficiency?
Correct
That’s what I would say. You’ve just crossed the threshold of moderate (500 ms for the pressure half-time.) But this is barely on the moderate side, so I agree that it would be reasonable to call it mild-to-moderate.
Incorrect
OK, maybe this is unfair. Reasonable people can disagree, and if you called this moderate you might not be wrong. I had called it mild-to-moderate because the pressure half-time was juuuust on the moderate side of mild (500 ms.)
-
Question 24 of 41
24. Question
What are we seeing here? Worried or not worried?
Correct
Yeah, you’d better be worried here. This short axis shows a significant coaptation defect in the aortic valve, you’d be surprised if there wasn’t significant AI. Whenever there is 2D evidence of a valve defect you know you’re in trouble.
Incorrect
Not exactly. Take another look and regroup. There is a large coaptation defect in the aortic valve, and you should expect significant regurgitation any time you see a 2D defect.
-
Question 25 of 41
25. Question
How bad is the AI?
Correct
Yes, you nailed another one! The first image is concerning for more-than-mild AI (meaning you’d like to spend more time quantifying.) When you measure the vena contracta it falls into the moderate range (3-6mm) which confirms your suspicion. How could you improve this vena contracta measurement? What other measures would be necessary to confirm?
Incorrect
Rats, I was sure you had this one! The first image looks like more-than-mild aortic insufficiency, meaning you’d like to spend some more time quantifying it. When you measure the vena contracta, it falls into the moderate range (3-6 mm) confirming your suspicions. How would you improve the vena contracta measurement here? What other information would you need to shore up your quantification?
-
Question 26 of 41
26. Question
What view is this and where is the arrow located?
Correct
This is a midesophageal aortic valve short axis. We see the left atrium at the top of the screen (under the transducer), which tell us that we’re in the mid esophagus, and we’re focused on the aortic valve. The arrow is pointing at the right coronary cusp of the aortic valve. Remember that the noncoronary cusp is always located adjacent to the interatrial septum and the right cusp is always by the right ventricle (you could say the left cusp is “left over” I guess.)
Incorrect
Whoops! You probably realize by now that this is a midesophageal aortic valve short axis. We see the left atrium at the top of the screen (under the transducer), which tell us that we’re in the mid esophagus, and we’re focused on the aortic valve. The arrow is pointing at the right coronary cusp of the aortic valve. Remember that the noncoronary cusp is always located adjacent to the interatrial septum and the right cusp is always by the right ventricle (you could say the left cusp is “left over” I guess.)
-
Question 27 of 41
27. Question
What view is this and where is the arrow?
Correct
This is a midesophageal aortic valve short axis. We see the left atrium at the top of the screen (under the transducer), which tell us that we’re in the mid esophagus, and we’re focused on the aortic valve. The arrow in this case is showing us the left coronary cusp of the aortic valve. Remember the right cusp is by the RV and the non coronary cusp is by the interatrial septum.
Incorrect
Rats! This is a midesophageal aortic valve short axis. We see the left atrium at the top of the screen (under the transducer), which tell us that we’re in the mid esophagus, and we’re focused on the aortic valve. The arrow in this case is showing us the left coronary cusp of the aortic valve. Remember the right cusp is by the RV and the non coronary cusp is by the interatrial septum.
-
Question 28 of 41
28. Question
What is shown by the arrow?
Correct
Exactly, well done! The non-coronary cusp is always near the interatrial septum.
Incorrect
Well, not exactly…remember that the non-coronary cusp is always by the interatrial septum and you’ll be on track.
-
Question 29 of 41
29. Question
Where is the arrow pointing?
Correct
Yep, you got it. Well done!
Incorrect
Not exactly, did I fool you? Remember that the non-coronary cusp will always be by the interatrial septum and the right coronary cusp will be by the RV and you should stay on track.
-
Question 30 of 41
30. Question
Where is the arrow pointing?
Correct
Yep, no problem. Well done!
Incorrect
Come back and try this one again. Remember that the non-coronary cusp is by the interatrial septum and the right cusp will by the RV.
-
Question 31 of 41
31. Question
Where is the arrow pointing?
Correct
Enough said, you got it.
Incorrect
Whoops, come back and try that one again!
-
Question 32 of 41
32. Question
Describe the pathology.
Correct
Well done! Definitely not enough AI to worry about (mild) but you should be worried about AS here and will want to go on to quantify.
Incorrect
Not exactly. This is definitely not enough AI to worry about (mild) but you should be worried about AS here and will want to go on to quantify.
-
Question 33 of 41
33. Question
Describe the pathology.
Correct
Perfect, you got it!
Incorrect
Nope, time to review cutoffs for pressure half time in AI. The better the valve works the slower blood comes in (cutoff between mild and moderate is 500 ms.)
-
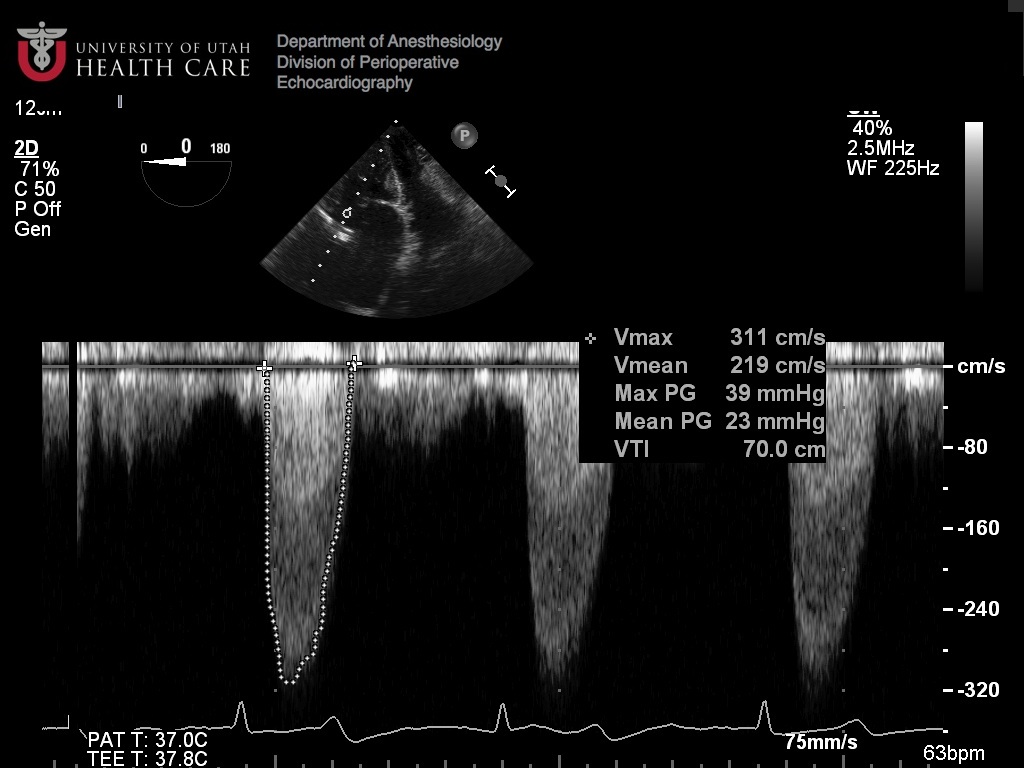
Question 34 of 41
34. Question
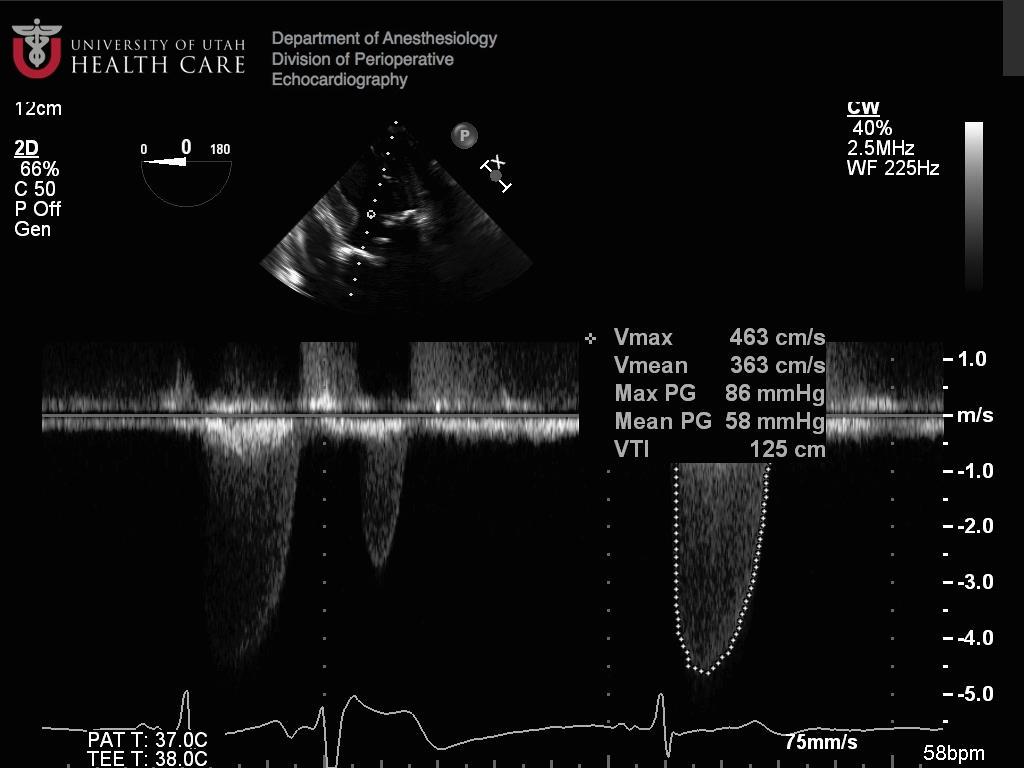
Describe the pathology.
Correct
Boom, you nailed it!
Incorrect
Must have been a mouse malfunction. This continuous wave doppler shows us two characteristics of severe aortic stenosis. Mean gradient > 40 mmHg, and peak velocity > 4 m/s.
-
Question 35 of 41
35. Question

Describe the pathology.
Correct
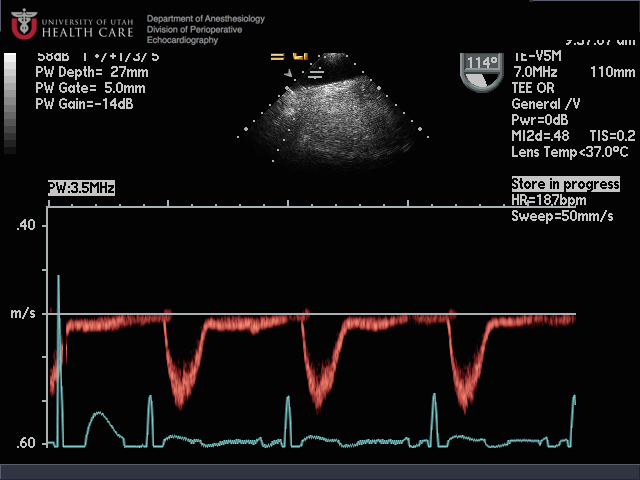
Can’t fool you, huh? You’re worried based on the color flow, but cannot quantify AI easily because it is severely eccentric. But the PWD in descending aorta confirms severe AI.
Incorrect
Well…no, not exactly. The color flow shows a concerning amount of AI, though you cannot quantify it easily because it is terribly eccentric. But the holodiastolic reversal of flow in the aorta confirms severe AI.
-
Question 36 of 41
36. Question
Describe the pathology.
Correct
Well done! Mild aortic insufficiency, don’t really need to quantify further when there is such a small amount of regurgitation.
Incorrect
Must have had a brief absence seizure, hope you’re better now. This is clearly a small amount of AI, you don’t really need to quantify further.
-
Question 37 of 41
37. Question
Describe the pathology.
Correct
Well done! Mild aortic insufficiency, both by CFD appearance and by PHT. Piece of cake.
Incorrect
Take a second to review these images again, and check your numbers. This is mild AI by both CFD and PHT.
-
Question 38 of 41
38. Question
Describe the pathology.
Correct
Well done! Mild aortic insufficiency, nuff said!
Incorrect
Nope, not this time. This is just mild AI.
-
Question 39 of 41
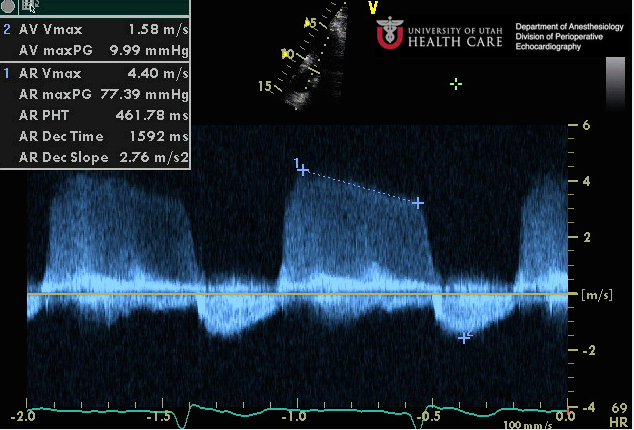
39. Question
Describe the pathology.
Correct
Exactly. With this information alone, you would have to call this moderate AI based on PHT.
Incorrect
Another slip of the mouse, you’d better get that thing checked. If this is all you have, you have to call it moderate AI (between 200 and 500.)
-
Question 40 of 41
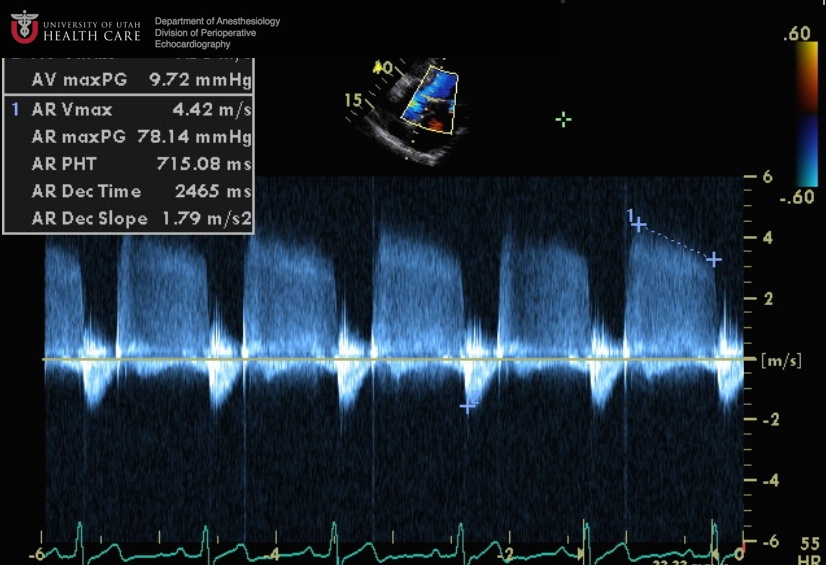
40. Question
Describe the pathology.
Correct
Well done! You’d definitely want more information here, moderate is the toughest call to make. But that’s what this is, I promise. Think of 5 ways to quantify further…
Incorrect
Rats, you missed it! It is tough to call moderate, and you would want to confirm with multiple other modalities. Think of 5 ways to quantify further…
-
Question 41 of 41
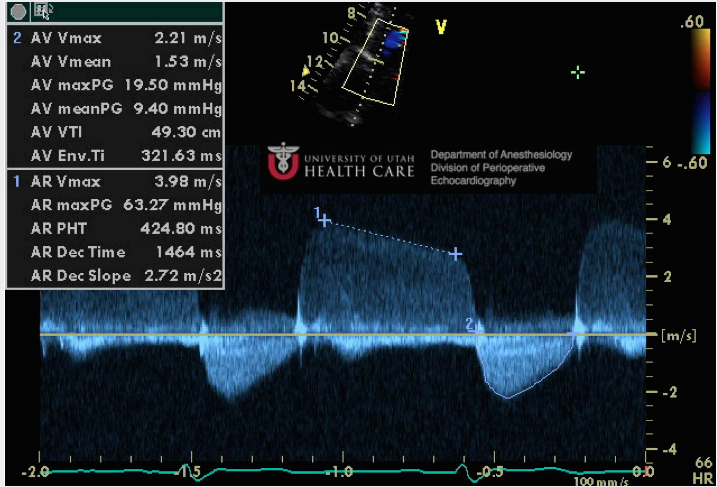
41. Question
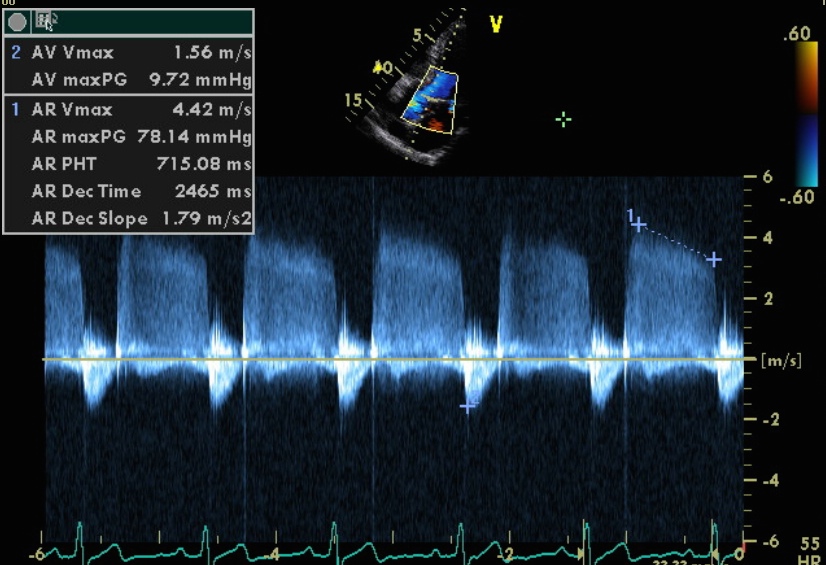
Describe the pathology.
Correct
Well done, my friend.
Incorrect
Nope, take another look at methods to quantify aortic insufficiency. PHT 200-500 with no reversal of flow = moderate.